The Efficacy Of Everything In Psychiatry In One Graph Plus Several Pages Of Dense But Necessary Explanation
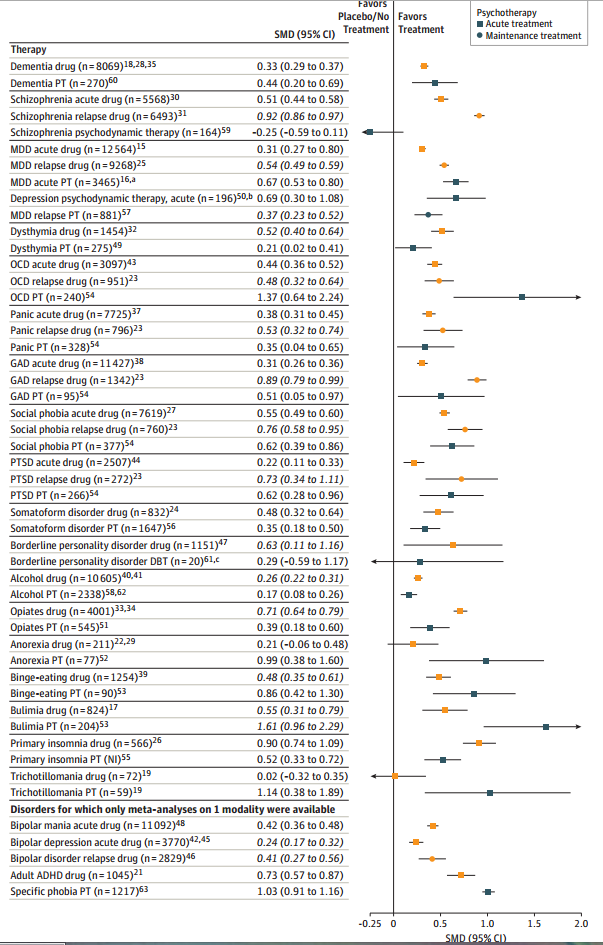
Shamelessly stolen from my hospital’s Journal Club: Huhn et al (2014) graph the Efficacy Of Pharmacotherapy And Psychotherapy For Adult Psychiatric Disorders, and it looks like this:
 Before anything else – we kind of have to assume that in each case they’re getting a representative sample of the best drugs/therapies for the disorder. In practice, there is this weird equivalency for most things: most common antidepressants work about equally well, most common antipsychotics work about equally well, et cetera. I don’t know as much about therapy, but I get the impression the same thing goes on there too. So probably it’s not much of a stretch to expect that the efficacy of whatever they studied at least kind of translates to the effectiveness of whatever real treatment you’ll get from your own psychiatrist. At the very least, even lossy and compressed information like this will tell us something.
Before anything else – we kind of have to assume that in each case they’re getting a representative sample of the best drugs/therapies for the disorder. In practice, there is this weird equivalency for most things: most common antidepressants work about equally well, most common antipsychotics work about equally well, et cetera. I don’t know as much about therapy, but I get the impression the same thing goes on there too. So probably it’s not much of a stretch to expect that the efficacy of whatever they studied at least kind of translates to the effectiveness of whatever real treatment you’ll get from your own psychiatrist. At the very least, even lossy and compressed information like this will tell us something.
The effect sizes are mostly around 0.5, with a few much higher and a few much lower. This is common for these sorts of studies. See for example Leucht et al, Putting the efficacy of psychiatric and general medical medication into perspective, which also finds psychiatric effect sizes average around 0.5 and finds this is about equal to average effect sizes in other fields of medicine – thus debunking the popular claim that psychiatry is less effective. Leucht and a few other authors from that piece are also involved in this one, which doesn’t surprise me much.
I do however admit my statistical ignorance in exactly what is going on here. Effect sizes are a good way to compare two unlike domains – for example, I recently noted that leading physicists are about as smart as NBA players are tall. This paper is within that tradition. In fact, if we wanted, we could describe psychiatric medications as about one-sixth as effective as NBA players are tall. This is perfectly honorable. The height of NBA players is a tough bar to live up to.
But I don’t have a good intuitive feel for what it means to use standard mean differences along a non-normally distributed variable – as psychiatric diseases no doubt are. And I’m not sure where they’re even getting their distributions from. When they say schizophrenia meds have an effect size of 0.52, are they talking about the distribution of the general population, with almost everyone near zero and a few schizophrenics way off to the right? Are they talking about the distribution of how schizophrenic particular schizophrenics are, which for all I know might be a bell curve but which is probably very different depending on how you took your schizophrenia sample? I really don’t get this and it’s preventing me from getting a good feeling of exactly how comparable these numbers are to each other.
If we just assume they’re allowed to do what they’re doing, their graph looks about how I would expect it to look. Most psychiatrists always figured that the psychotic disorders were more susceptible to medication and the anxiety disorders to psychotherapy. But three surprises stand out.
First, this graph shows that drugs are more effective than therapy in treating borderline personality disorder. That’s the opposite of the conventional wisdom, which says that some drugs can decrease impulsiveness in this population but that the definitive treatment has always been Dialectical Behavioral Therapy. But it looks like their borderline psychotherapy “meta-analysis” had a sample size of 20 patients (I would hate to see what the individual studies had!) compared to thousands of patients for most of the believable results. So I wouldn’t place too much faith in this anomaly for now and would continue to recommend psychotherapy for borderlines.
Second, this graph shows that drugs are more effective than therapy for insomnia. Now, we use drugs instead of therapy for insomnia, but conventional wisdom had always been that this was very sad, and there was great therapy available for insomnia if only somebody would provide it. But here the therapy looks mediocre at best. On the other hand, the sample size is “NI”, which I don’t know what it means but doesn’t sound promising. Also, now that anticholinergics probably cause dementia, every single sleeping pill now officially has terrible side effects.
Third, in all conditions drugs seem more effective at preventing relapse than at stopping acute episodes. My “clinical experience,” which is the fancy word doctors use for anecdotal evidence, was exactly the opposite. I now realize I probably faced a lot of selection bias – the patients who do well on their drug and don’t relapse might never see me again. Also, I have a feeling that a lot of the people who come back to me a month later and say “Well, your drug must not have worked, I’ve relapsed again” probably weren’t taking the drug correctly or at all, something which these studies probably enforce better than I can.
In general, the table seems to support psychotherapy being better than drugs for a lot of things. This would not be too surprising if true – their list is heavily tilted to the kinds of conditions therapy works well on – but a caveat is necessary.
The psychotherapy trials were generally of lower quality. Part of this has to do with the culture of psychotherapy research, but more has to do with the underlying territory – giving people “placebo psychotherapy” is more complicated than giving people a sugar pill and a lot of studies don’t bother. Also, in psychotherapy, it tends to be the patient’s therapist recording results more often than corresponding pharmacology studies use the prescriber to record results. That eliminates another layer of blinding.
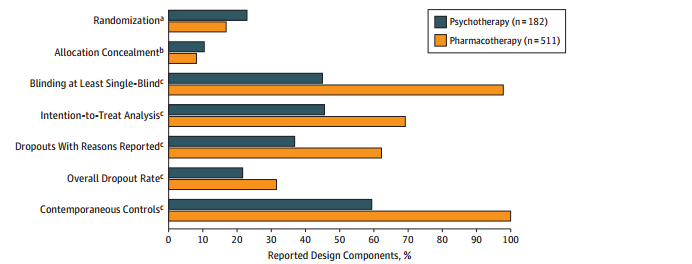 This has serious ramifications. The study finds that “low-quality psychotherapy trials in general had a higher effect size (SMD = 0.74) than high-quality trials (SMD = 0.22), p < 0.001". Those high effect sizes for psychotherapy aren't looking so good now, are they?
This has serious ramifications. The study finds that “low-quality psychotherapy trials in general had a higher effect size (SMD = 0.74) than high-quality trials (SMD = 0.22), p < 0.001". Those high effect sizes for psychotherapy aren't looking so good now, are they?
Actually, reread that one more time. Effect sizes for the low quality trials are triple those for the high-quality trials. If you ever wanted proof that it’s way too easy to inflate positive findings if your science isn’t really exceptionally good, there you go.
The most important domain where pharmacotherapy trials are worse than psychotherapy trials is publication bias. The paper suggests that this is because psychotherapy’s lack of sufficient blinding and control groups makes publication results unnecessary. In other words, psychotherapy research isn’t even good enough to have publication bias, because publication bias at least requires you to be rigorous enough to occasionally turn up a negative result to suppress. Ouch.