[ACC Entry] Should Childhood Vaccination Be Mandatory?
This is an entry to the Adversarial Collaboration Contest by Mark Davis and Mark Webb, who sent the following introduction along with their entry:
Mark Davis is a naturopathic doctor. Naturopathic medicine is a century-old profession in the United States, but it’s small, with fewer than 10,000 NDs licensed to practice naturopathic medicine in the US in 2018. The profession has been historically highly skeptical of vaccination in general, and the modern profession is contentiously split on the topic, with vocal advocates of CDC-scheduled routine childhood vaccination and vocal dissidents both offering continuing medical education for NDs. Mark Davis’ main goal in this adversarial collaboration was to argue that there is enough reasonable doubt that routine childhood vaccines could contribute to hyper-inflammatory disease, and enough reduced harm from vaccine-preventable diseases from other medical and public health interventions (in countries with greater economic resources) that parents should be given wide latitude to make individual choices re: routine childhood vaccines despite the clear benefits to individual and public health from preventing those diseases. He became more convinced in his conversations with Mark Webb that widespread childhood vaccination is in the best interest of public health.
Mark Webb is a clinical researcher – with a current focus in oncology. He completed a PhD in immunology, specifically focused on the mechanisms driving the development of asthma. Mark Webb’s main goal in this collaboration was to argue that atopy and autoimmunity are likely not driven by vaccination, and that this idea is a distraction from finding the real causes of the increase in these diseases. Throughout the collaboration, he was reminded of the nature of safety surveillance with all drugs, and of the sensitive nature of vaccination as a medical intervention. He became persuaded that policy should not just reflect the best evidence currently available, but should also reflect a certain degree of humility that there will always be something we don’t know.
Setting the parameters of the debate
Why are vaccines the target of both intense support on the one side, and intense skepticism on the other? In part, this is because of the nature of how vaccines work. On the side supporting vaccination, there is strong evidence that vaccination changed the face of epidemic disease in the 20th century. Smallpox is effectively extinct, and polio is nearly there. What agent caused this veritable miracle? Vaccines did. Some diseases are harder to create vaccines against, like HIV or herpes, but eventually we can envision a day when vaccine development can – not just cure – but prevent huge numbers of people from ever having to worry about the deadly diseases of the past. Vaccination is clearly a proven tool for promoting public health. It has been successful at eradicating diseases that used to be endemic to various regions; and where diseases haven’t been eradicated vaccination has been very successful at preventing outbreaks and disease spread. What could possibly be bad about vaccination?
Perhaps the biggest reason vaccination has received the degree of skepticism it does is because of how it is administered. Any medical intervention that is targeted toward a high percentage of the population should be scrutinized. Indeed, it would be irresponsible not to undergo continual safety surveillance of a medical intervention that is administered to 90% or more of the population. Vaccines are also administered in multiple doses to one of the most vulnerable population categories: children. There is a strong tradition in clinical research to ensuring high levels of oversight toward children and other vulnerable populations.
Finally, vaccination is a medical intervention intended to produce a permanent effect. It is especially important to be vigilant about therapies whose effects are intended to be persistent. A drug that temporarily relieves asthma symptoms is generally less suspect than one that actually cures asthma. This is because if the expected effects disappear over time, any unknown and unexpected effects are more likely to disappear (although this is not always the case). However, if we’re looking at a treatment with long-lasting effects, unknown long-lasting effects could also appear.
This does not, in itself, mean we shouldn’t implement medical innovations meant to be permanent, targeted toward children, or that would have widespread impact. That would be like suggesting we cease all pediatric cancer research. But it is important to understand why the conversation about vaccine safety is necessarily an ongoing inquiry, not a one-off check of whether “vaccines are safe”. It is also not irrational for a subset of individuals to continue to be wary of possible missed adverse effects, no matter how much research fails to demonstrate any harm.
Before we introduce the parameters of this debate, we wish to emphasize that vaccination is a method of intervention, not one specific intervention. The statement “vaccines are safe” cannot be applied across the board to all vaccines that ever have or ever will be created, any more than you could say, “prescription drugs are safe” for all current and future prescription drugs. This question would hinge more on our confidence in the clinical approval process to ensure drug safety – an interesting question, but one entirely beyond the scope of this essay. In that sense, any general complaint you might make about prescription drug approval or safety could equally apply to any vaccine. In addition, a dozen studies demonstrating the safety of the DTaP vaccine do not demonstrate that MMR is safe. Studies for MMR have to be conducted independently, just as studies about amlodipine do not tell us whether olmesartan is safe.
These, then are the parameters surrounding vaccine safety:
- Vaccination has proven benefits to public health
- Vaccination has all the hallmarks of an intervention with the potential to cause harm
One more consideration should be noted here. In general, the benefits of widespread adoption of routine childhood vaccination in countries with fewer economic resources are clear and not disputed between the collaborators. Nations with little access to medical care are likely to see greater benefits from vaccination than nations with highly accessible medical care infrastructures. For example, an infection that would be lethal in parts of sub-Saharan Africa might be easily treated if contracted in France. Thus, a risk-benefit analysis for economically developed countries will require a more stringent requirement for clear benefit over risk than in the developing world.
From this, we will consider two proposals for economically developed nations such as the US, Europe, Canada, Japan, etc.:
- Mandatory vaccination is necessary to achieve public policy objectives for vaccines.
- Public policy should encourage parents to not vaccinate, or should at least normalize parents’ decisions to avoid vaccination.
Should vaccination be mandatory?
In order to recommend that vaccination, as a matter of public policy, should be mandatory, we would need to show that:
- Vaccination achieves a legitimate public policy objective
- This public policy objective cannot be achieved without making vaccination mandatory
When considering vaccine benefits (and indeed virtually everything about vaccines) it is important not to generalize the best or worst aspects of one vaccine with another vaccine, or a vaccine used in one socio-economic context with a vaccine used in another. The benefits of the smallpox vaccine have been significantly greater than, say, the rotavirus vaccine, and rotavirus vaccine provides more benefits in countries with few healthcare resources. Even so, rotavirus vaccination still conveys positive benefits that should not be ignored; those benefits should simply be put in context, and any potential adverse effects of rotavirus vaccination should be factored in.
Let’s continue with rotavirus for a minute to highlight what we mean. In most people who contract rotavirus, the greatest concern is dehydration. Most deaths from rotavirus currently occur in the third world, not because rotavirus isn’t transmitted in the US, but because among those who do contract rotavirus hydration therapy is highly successful. In other words, if you’re living in a place where you have to hike 3 miles to collect dirty drinking water that made you sick in the first place, you’re going to struggle with this disease. If you live in Germany and have ready access to quality healthcare services no matter where in the country you live, you’re probably going to be fine.
That doesn’t mean the rotavirus vaccine does nothing. Most people who get the vaccine will be spared the debilitating diarrhea and possibly the trip to the ER. So it’s a meaningful intervention, but it’s not really a life-or-death intervention in resource-rich countries. A similar story can be told for some – though not all – of the other vaccines on the US CDC’s recommended schedule. Generally speaking, not contracting the disease produces the positive good of preventing morbidity and other costs to individuals, but it’s mostly not a life-or-death event. This distinction is important, because “has strong benefits” can be weighed against potential downsides. On the other hand, “keeps you from dying” is hard to weigh against even debilitating or disfiguring downsides. This is basically how something like chemotherapy can become a real treatment, instead of a particularly cruel “enhanced interrogation” technique.
If you live in a totalitarian dictatorship, it’s much easier to make something mandatory. You just tell everyone to do it and if they don’t, you line them up against the wall. In a democratic republic, where the perception of the people often shapes public policy, it’s important not to make enemies of the general public. And although this is not a bar against a mandatory policy, it suggests any such policy should be tempered with the aim of ensuring it is strongly justified, is not rigidly unyielding, and therefore does not become burdensome and unpopular. In the US, in most states, mandatory public vaccination tends to meet this bar (with some qualifications).
First, the policy is not rigidly unyielding in most states. Every state in the USA has some form of mandatory vaccination policy in order for children to attend public schools. Since education is mandatory, and public schooling is freely available to all children, this amounts to a strongly coercive opt-out system. Parents who do not wish to vaccinate are forced to pay a price for their dissention by finding some other way to educate their children than through the public education system they cannot opt out of contributing to through taxation.
Some exceptions are allowed, depending on the state you live in. For example, every US state allows exemptions for medical reasons, since, for example, some small percentage of people are allergic to some of the components of vaccines. All but three states allow religious exemptions, for those whose religion prohibits vaccination (CA, MS, and WV only allow medical exemptions, representing less than 15% of the total US population). But if you don’t belong to a religion that prohibits vaccination, you’ll need to live in one of the 18 states that allow exemptions for personal beliefs as well (these include AR, AZ, CO, ID, LA, ME, MI, MN, MO, ND, OH, OK, OR, PA, TX, UT, WA, and WI representing about 35% of the US population) if you want your children to attend public school without getting them vaccinated.
There is, perhaps, a general concern about totalitarian tendencies here. The concern is that, with physicians as gatekeepers of medical care, they are in a particularly coercive position when it comes to individual patient decisions. Say a patient is strongly opposed to some aspect of vaccination, and wants to opt out of the system. When they try to do this, perhaps their doctor refuses to play along, preferring to use their position of authority to compel the parents to following standardized guidelines. This is certainly the case in some situations, but is it the norm? According to a survey of Washington State pediatricians in 2011, a majority reported they are willing to follow an alternative vaccination schedule to the one advocated by the CDC if a parent requests one. Interestingly, 77% of the pediatricians surveyed reported parents sometimes or frequently make these requests. So not only are parents asking pediatricians to follow different guidance than what the CDC recommendations, most pediatricians report that they are willing to comply. As these are statistical results, this means that there are some parents asking to follow a different vaccine schedule who are refused by their pediatrician; but it appears that (at least from what we know of Washington State) these parents need only go looking for a readily-available second opinion and they will find a pediatrician who is willing to go along with the vaccine schedule they prefer.
Despite this, the argument, “vaccination should be mandatory” must contend with one uncomfortable fact: in many European nations vaccination isn’t mandatory, and those nations often achieve higher vaccination rates than in the US. The table below lists different nations’ vaccination rates. In addition to comparing these rates to one another, it is necessary to compare rates to the threshold required for “herd immunity”. One compelling public health argument in favor of vaccination is the potential of a vaccine to stop the spread of a disease because an infected person will be unlikely to spread the infection prior to recovery because everyone they meet is already immune. It’s a little more complicated than this, but fortunately it can be easily simplified into one number that represents the percentage of the population that needs to be vaccinated in order to ensure the disease will slowly die out faster than it can spread. This is represented by the “threshold” row in the table below.
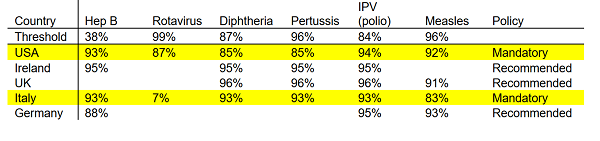 Notice that for hepatitis B less than 40% of the population needs to be vaccinated in order to achieve herd immunity. Hepatitis B is usually the first vaccine babies get, with current recommendations being to give this prior to leaving the hospital. The specifics of why this vaccine is recommended this early are probably beyond our scope, but from the perspective of “intended to stop the spread of the disease” we’re probably more aggressive than we need to be. Meanwhile, for rotavirus nearly everyone has to get the vaccine in order to achieve herd immunity. We’d have to live in a totalitarian dictatorship to get the kind of levels we’d need to eradicate rotavirus through vaccination alone. It’s important here to note that the vaccine does confer protection to an individual who receives it. But since rotavirus is so highly contagious, really high vaccination rates are not enough to stop the spread of the disease. Thus, as a personal healthcare decision the rotavirus vaccine appears highly attractive. However, as a matter of public policy rotavirus vaccination cannot be expected to prevent outbreaks. It might make them a little less severe, or perhaps they’ll spread more slowly, but they’ll still happen.
Notice that for hepatitis B less than 40% of the population needs to be vaccinated in order to achieve herd immunity. Hepatitis B is usually the first vaccine babies get, with current recommendations being to give this prior to leaving the hospital. The specifics of why this vaccine is recommended this early are probably beyond our scope, but from the perspective of “intended to stop the spread of the disease” we’re probably more aggressive than we need to be. Meanwhile, for rotavirus nearly everyone has to get the vaccine in order to achieve herd immunity. We’d have to live in a totalitarian dictatorship to get the kind of levels we’d need to eradicate rotavirus through vaccination alone. It’s important here to note that the vaccine does confer protection to an individual who receives it. But since rotavirus is so highly contagious, really high vaccination rates are not enough to stop the spread of the disease. Thus, as a personal healthcare decision the rotavirus vaccine appears highly attractive. However, as a matter of public policy rotavirus vaccination cannot be expected to prevent outbreaks. It might make them a little less severe, or perhaps they’ll spread more slowly, but they’ll still happen.
The important observation from the table above, however, is that nations like Ireland and the UK have much higher vaccination rates than the US without making them mandatory. Often, these rates are much higher. For example, the US rate of vaccination against diphtheria is below what is required to achieve herd immunity, in contrast to diphtheria vaccination rates in Ireland and the UK, which exceed the level required for herd immunity. This is not to say that eliminating mandatory vaccination will increase vaccination rates. Each nation has different, and unique, health care systems, laws, policies, and behavioral norms. This is probably more complicated than “Let’s just copy what the Germans are doing.” But it is not possible to argue, “Without mandatory vaccination we cannot achieve herd immunity; people will be dying of disease in the streets!” Although we should be cautious about sudden, dramatic changes to a system that is largely working, both authors concede that in developed nations such as the US mandatory vaccination is probably not necessary to achieve public health objectives.
Should health authorities normalize parental decisions not to vaccinate?
Any medical intervention comes with some level of risk, both known and unknown. For vaccination, the most common, well-documented, known risk is the potential for an allergic response to some component of the vaccine. The most common allergic component is egg, and people with severe egg allergies are instructed to consult their physician prior to vaccination. How common are allergies to vaccines? A good estimate is about 3 per one million doses. This would be the equivalent of about 200 people in France, or 35 in the US state of Ohio. This is the biggest recognized, known risk of vaccines. But are there significant unrecognized risks of vaccination that could impact the risk/benefit assessment of vaccine safety?
In order to make a general recommendation against vaccination as a matter of public policy, any identified harm would need to outweigh the benefits which those vaccines confer upon their recipients. There are a number of theories about potential harm that could come from vaccines. Much ink has been spilled about vaccines and autism, and it is not our intent to cover that ground again here. Both authors agreed that the evidence does not support a link between vaccines and autism.
There is another, more subtle linkage that we would like to consider here; this is the hypothesis that vaccines might contribute to autoimmune and autoinflammatory diseases such as multiple sclerosis, type I diabetes, inflammatory bowel disease, rheumatoid arthritis, etc., or to atopic diseases such as asthma, eczema, and food allergies. These diseases have been increasing for decades – the same decades during which we have increasingly been administering more vaccines, earlier and earlier in childhood and into infancy. Thus, it is appropriate to consider the possibility of a causal link between these two phenomena: do vaccines lead to autoimmune and allergic disease?
Are kids who are vaccinated more likely to develop these immune system diseases? Despite a large number of studies into this area, the results so far have been mixed. On one hand you could argue, as above, that vaccines lead to increases in immune system diseases. And indeed, you can find researchers who have demonstrated just such a link for DPT, tetanus, MMR, etc.
- DPT (article; article)
- Tetanus specifically
- Tuberculosis (BCG vaccination doesn’t prevent allergic disorders, but positive TB test does)
- Measles (article; article)
Meanwhile, other researchers have hypothesized that vaccination protects against development of allergic disease and autoimmunity. How might this be? There is strong evidence that increased antibiotic use in early childhood is associated with increases in developing immune system diseases; childhood use of antibiotics can shift the balance of commensal bacteria in a way the hygiene hypothesis would predict makes you more susceptible to immune system diseases. So it’s also possible that not vaccinating could lead to increased antibiotics use if your child does get infected with measles, mumps, pertussis, etc. Regardless of whether antibiotics are the mediating factor, some studies indicate certain vaccines having a protective effect against atopy:
- Tuberculosis (meta-analysis)
- Measles (article; article)
- MMR (article)
Finally, some studies find no difference between vaccination and natural infection in development of immune system disease:
- Multiple vaccines (article; article)
- DPT (as a marker for all vaccines)
- Pertussis (We were only able to locate one genuine placebo-controlled RCT of a routine childhood vaccine in which the authors looked for atopy – they found no significant difference in atopy between the placebo and real pertussis vaccine groups at ages two and a half and seven)
This topic has been reviewed multiple times in the scientific literature, and the conclusions have been the same each time: there is no demonstrable impact of vaccines driving immune system diseases. Given these conflicting studies, we can’t say that there is convincing evidence that vaccines either cause increased immune system disease or that they protect against development of these diseases.
One hypothesis for how vaccines might contribute to the rise in atopy and autoimmunity side-steps most of the evidence cited above. These articles look at whether vaccination itself causes allergic disease, but what if the opposite is true – not vaccinating protects against allergic disease?
Hygiene Hypothesis
What causes the development of autoimmune, autoinflammatory, and atopic disease? A full answer to that question – one that could lead to prevention of these diseases – would probably be worth at least a Nobel prize in medicine; which is to say we don’t entirely understand it. However, the current leading explanation in vogue amongst immunologists and epidemiologists who study the recent trend in which we see these diseases increasing dramatically in the developed world is call the hygiene hypothesis.
First proposed about thirty years ago, the hygiene hypothesis is the idea that some of the bacterial and parasitic infections that modern medical technology has eliminated might have been performing an important function in the human immune system – and when you take them away you start seeing problems. For example, if you go back 5,000 years in human history, few people would be completely free of parasitic infections, such as hookworm or whipworm. These parasites might make you mildly ill after you first get infected, but so long as your immune system maintains control of the infestation you may not notice it. There is a constant, low-grade battle between your immune system and the parasite. This battle doesn’t just go on your entire life, but has gone on for generations of humans (and their common ancestors), such that this is the normal state of affairs. Fast forward 5,000 years, and modern water treatment suddenly prevents millions of people from ever experiencing a type of infection that was a constant throughout humanity’s evolution. As a result, the immune system doesn’t know what to target. There has never been a time when there was nothing to fight, so it begins to fight itself, accidentally.
This hypothesis isn’t just high-level theoretical hand-waving. Parasites, such as hookworm, have been shown to induce the same kind of immune mediators that are commonly seen in autoimmune diseases. In fact, some people with diverse autoimmune, allergic and autoinflammatory conditions have started intentionally infecting themselves with hookworm. Based in part on this movement, clinical trials have been conducted, and more are currently under way investigating whether re-introducing parasitic infections such as hookworm can be used to treat Crohn’s and other autoimmune diseases.
If the hygiene hypothesis is correct, and removing certain persistent infections is driving the increase in autoimmunity, autoinflammation, and atopy; does that mean there is a hygiene hypothesis explanation that links vaccination with these diseases?
This hypothesis is much more difficult to test, in the case of vaccination, because it’s not saying the vaccine itself causes allergy and autoimmunity. Instead, it argues that getting rid of diseases such as measles and pertussis causes the increase in allergy and autoimmunity. Thus, it doesn’t really matter whether you get the vaccine or not, what matters is whether you get measles or pertussis or not. If everyone around you gets vaccinated, herd immunity will kick in – the very effect public policy is looking to achieve – and you will never get the chance to catch measles. So no matter how large or well-designed or randomized/controlled, a study that compares US children who are vaccinated with those who aren’t won’t be able to test the hypothesis that endemic measles outbreaks protect against development of allergies and autoimmunity.
The closest we can come to addressing this question are some of the measles studies cited above. One of these compared individuals in Guinea-Bissau who were either naturally exposed to measles or who had been vaccinated; they identified a protective effect for natural measles exposure. Meanwhile, another study in Finland made a similar comparison and found natural measles infection exacerbated atopy and allergic disease. The problem with this approach is that it doesn’t just compare vaccination with not vaccinating – it compares people who don’t vaccinate with those who do. These are not necessarily the same. For example, people with access to vaccines in a nation such as Guinea-Bissau might be of a different socio-economic status than people with no access to vaccines. And socio-economic status has been identified as a factor in development of atopy and autoimmunity.
One way to look at this is to ask whether vaccinated children have different immune system markers, such that they look like they are more susceptible to developing immune system diseases. Researchers at the University of British Columbia looked for exactly this kind of change in a recent study. They took blood from children who had or had not been vaccinated and looked at whether these children’s circulating immune system cells differed from each other. They did not find any of the differences we would expect to find if vaccines caused a general shift in a vaccinated person’s immune system. This study should be taken with a large grain of salt however, as the sample size was smaller than expected, due to the difficulty of recruiting unvaccinated children.
A more targeted way to test this hypothesis would be to randomly assign children to receive one or multiple vaccinations and compare to children who receive no vaccination, then expose all the children to the disease(s) they were vaccinated against and check whether they develop various types of atopic and autoimmune disease. This would have to be done in a nation that currently has endemic levels of the disease in question and/or frequent outbreaks. Also, a nation with no scruples about conducting experiments on children in which you intentionally expose them to infectious agents at an early age.
This does not mean the hypothesis cannot be tested, but it will be a difficult hypothesis to test consistently, and the current state of the evidence suggests a high level of disagreement. In advance of such evidence, we might ask: What are the implications if this hypothesis were confirmed? Would that mean deciding whether to accept – even encourage – endemic disease burdens such as measles, polio, pertussis, etc.? There is no reason to believe that the hygiene hypothesis requires specific bacterial or parasitic infections in order to promote the development of a healthy immune system. It is likely that whole classes of commensal bacteria are protective against the development of atopy and autoimmunity. If there were a group of people, living in a nation that has achieved herd immunity to many of the infectious agents discussed above, and that had rates of allergy and autoimmunity significantly below that of the rest of the population we might study that group to determine whether they are exposed to commensal agents that are protective against atopy and autoimmunity.
Fortunately, the Amish in the US provide an excellent example of just such a case. They experience almost none of the diseases we associate with developed nations. They have far less cancer, asthma, food allergies, MS, etc. You might think, “but that’s because they don’t vaccinate!” except that they do vaccinate. Different communities vary, as each Amish community makes its own rules about what aspects of modern technology to adopt, but one survey of the Amish suggests that about 85% of Amish children are receiving vaccinations. Additional anecdotal evidence suggests this may be a lower bound, but even if we assume 85% of Amish children are getting vaccinated we have to wonder why they see such low rates of modern diseases. Sure, they aren’t at the 90-95% of most of the rest of the country, but it’s hard to see how that extra 5-10% vaccination rate could be leading to such a huge increase in autoimmune diseases – especially without significant numbers of outbreaks running through their communities. Maybe it’s just something about the Amish?
It’s not just something about the Amish. An early observation about the hygiene hypothesis is that people who live on farms have a much lower rate of developing immune system disorders. The belief is that this is because they are more frequently exposed to environmental bacteria and parasites.
A group of researchers identified a different German religious sect, called the Hutterites, which also engages in regular farming. They are closely related to the Amish, and came from similar parts Germany at similar times. However the norms of the Hutterites dictate a much lower interaction between livestock and children/pregnant women (most hygiene hypothesis evidence suggests prenatal, neonatal, up through young childhood exposure is the critical exposure period). This genetically similar group, who had less early-life exposure to the farm environment than the Amish, gets asthma at a rate 5-7 times higher than Amish farmers (Amish asthma rate is 2-3%, Hutterite asthma rate is 15%). The researchers then took dust from the Amish barns and forced mice to breathe it in. They found the dust protected the mice from developing an experimentally-induced allergic response, and that it caused real, measurable changes in the immune systems of these mice, consistent with what we see in humans who are less allergic, and consistent with the differences they saw in the Amish farmers who had low allergic disease compared to the Hutterites.
But not everyone can live on farms (anymore) so current research is also focused at discovering which commensal bacteria humans need to protect against developing immune system diseases. This is similar to the idea of taking the dust from Amish farms, but consistent treatments require us to actually know what elements of the dust actually matter to preventing disease. It’s possible, for example, that modern lifestyles reduce exposure to exposure to mycobacteria. Some promising attempts have been made at reintroduction of killed mycobacteria into atopic individuals. This approach is akin to creating a vaccine against atopic disease, though more recent research has focused on changing the balance of live bacteria instead of simply introducing killed bacteria. This approach attempts to retrain the all-important gut commensal balance through techniques such as fecal microbiota transplantation (poop transplants) or investigating dietary changes that could help push the balance toward protective commensal bacteria and away from sensitizing commensals.
If we create a vaccine that specifically targets the commensal bacteria, or parasites that protect you from developing immune system diseases, we might suspect that vaccine of directly contributing to people who receive it developing those diseases. For example, one such helminth has been the target of recent vaccine development due to the significant harms it causes in the developing world; thus there is a concern on one hand of the persistent symptoms of infection caused by the hookworm infection, and a concern on the other of increasing the risk of allergic infection. In the developing world, where iron deficiency is a major cause of morbidity (large hookworm infections cause iron deficiency as they feed off the blood of hosts), development of an anti-hookworm vaccine could be a significantly beneficial intervention. In economically developed nations these types of infections were mostly eliminated when water treatment eliminated the fecal-oral route many pathogens use to spread from host to host.
Let’s revisit the implications of the hypothesis that the elimination of endemic diseases by vaccines causes an increase in atopy and autoimmunity. Currently, there is not strong evidence that vaccines drive autoimmunity and atopy, although additional research should be done in this area – focusing on disease exposure and not just vaccination status. Even if such a link were to be established in the future, is cessation of vaccination the best approach? Perhaps a better solution to the rise of atopy and autoimmunity is not to actively encourage the return of endemic diseases that are associated with other significant harms, but to encourage exposure to commensal bacteria and parasites that do not come with significant associated morbidity and mortality, such as those that help prevent atopy and autoimmunity in the Amish.
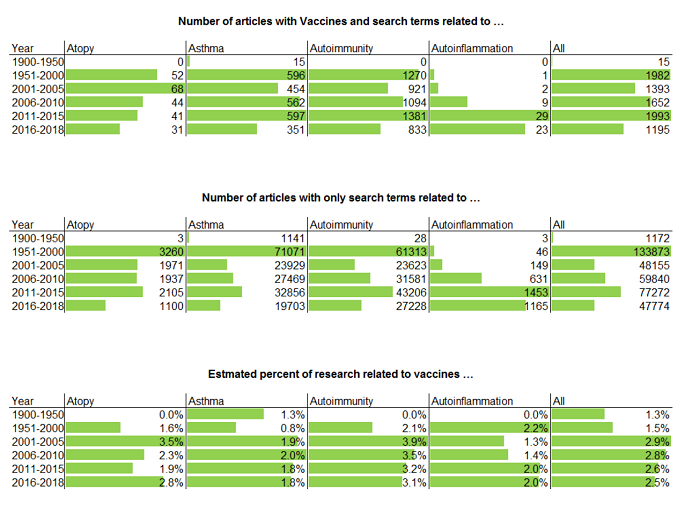
For the vaccines currently recommended today, we haven’t seen convincing evidence of long-lasting or permanent negative side effects. It is important that the medical community continue to monitor vaccines to confirm the relative safety of vaccination, and the evidence of the academic literature is that this is actively happening. Every year, many articles posted to PubMed confirm that ongoing surveillance of vaccine safety is being actively pursued by the scientific research community.
 This is appropriate, as we do not ever expect to finally “prove” that vaccines are not harmful. While it is possible to obtain support for a positive declaration such as, “vaccines are effective”, the only way to “prove a negative” with the scientific method is to fail to find support after looking for it. With vaccines, it is important to remember that this is a daunting task. There are many vaccines currently in use, and there are many possible harms to be investigated. In addition, new vaccines are currently being developed, such that we should expect to continue to investigate the safety of various specific vaccines for the foreseeable future.
This is appropriate, as we do not ever expect to finally “prove” that vaccines are not harmful. While it is possible to obtain support for a positive declaration such as, “vaccines are effective”, the only way to “prove a negative” with the scientific method is to fail to find support after looking for it. With vaccines, it is important to remember that this is a daunting task. There are many vaccines currently in use, and there are many possible harms to be investigated. In addition, new vaccines are currently being developed, such that we should expect to continue to investigate the safety of various specific vaccines for the foreseeable future.
Conclusions
In the first question, we assessed whether vaccination, as a matter of public policy, should be made mandatory. In essence, this asks whether the benefits to vaccination are sufficiently great that the decision of whether to vaccination should be removed from individual decision-making. Given the sensitive nature of a policy that essentially amounts to dictating private parental medical decisions, we adopted a standard similar to the US Supreme Court’s “strict scrutiny” standard: is it a compelling public health interest, and is it narrowly tailored? This is not generally the standard currently adopted by policy makers today. Mandatory vaccination failed this test, in that it is not narrowly tailored, since herd immunity can be achieved without making vaccination mandatory.
The case of California is an interesting example of how public policy is currently set in regards to vaccination. In 2014, California’s measles vaccination rate was below what is required for herd immunity, and there was a subsequent outbreak of measles at Disneyland. This was a high-profile event. In response, vaccine proponents argued that California’s laws should be strengthened to eliminate the personal and religious exemptions for vaccinations that were then in place. After the law was passed, despite a suspiciously large increase in medical exemptions, vaccination rates rose above the level required to achieve herd immunity, both at the statewide and at the county level. This law also sparked protests from parents who saw the law as removing the rights of parents to make medical decisions for their children. The debate was highly contentious, and continues to be a source of some political animosity.
According to our analysis, future public debates about vaccination do not have to follow this pattern. It is sensible, given the nature of vaccination as a medical intervention, to be skeptical that safety surveillance may have missed something important with respect to vaccines. It is also entirely possible to achieve vaccination rates sufficient to achieve herd immunity without removing medical decision-making ability from parents. A better approach might be to study models such as those of the UK and Germany. In the UK, vaccination is strongly recommended, and vaccines are provided at no cost to the individual. Germany, meanwhile, also strongly recommends vaccination but does not pay for vaccines. A more thorough study of social norms and other factors influencing vaccination rates could provide alternative approaches to the drive for mandatory vaccination, and help alleviate this front of the culture war. This study of alternatives to mandates should be undertaken prior to the next high-profile event, in order to provide policy-makers with a ready alternative that can foment good will between those wary of vaccination and those wary of the potential for outbreaks.
In the second question, we asked whether the public policy toward vaccination should be reversed. It is entirely understandable for concerned parents to adopt a “precautionary principle” approach to vaccination – given the nature of vaccination as a universal medical intervention targeted at babies and young children. However, as a matter of public policy, a general “precautionary principle” approach cannot be recommended in light of the proven harms vaccines protect against. At this time, there is not sufficient evidence that vaccination causes real harms – despite attempts to investigate various mechanisms by which they are theorized to cause harm. This does not mean vaccines cause no harm, but like any medical intervention, we require each vaccine to undergo initial testing for safety and efficacy before regulatory approval, then additional surveillance afterward.
Based on what we currently know, vaccines are an important element of disease control and eradication. Public policy may not require mandatory vaccination, but including recommendations for parents to vaccinate children is a legitimate public policy objective. Vaccine safety and vaccine surveillance are also important and legitimate. Many primary research articles are published each year investigating vaccine risks, and looking for unknown harms.
Ultimately, the question of whether something is “safe” can only ever be either answered:
- “no, we have evidence that it causes significant harm” or
- “we don’t have evidence that it causes significant harm”.
Meanwhile, many of the potential benefits of vaccination are recognized at the level of community adoption – which introduces a coordination problem. Thus, the central conflict we encounter in this area is between individuals who wish to invoke the precautionary principle for themselves and for their families, versus community standards that seek to eliminate a known danger. This conflict (between individual freedom to dissent in order to avoid fat-tailed risk versus a level of community solidarity necessary to combat societal ills) is common to many problems besides vaccination.
We believe this coordination problem may be largely resolved without restricting individual freedom. Individuals who wish to invoke the precautionary principle for themselves and their families should not be penalized for doing so.